
Fever is probably the oldest recognized sign of disease. Its study, description and interpretation dates from the earliest manifestations of civilization (1). And yet, today we lack common criteria to define the border of febrile temperature and its clinical management (2). In this whitepaper we discuss fever in both general and medical terms. We will also point out some issues that need addressed and why we think measuring the temperature of the blood that flows through the temporal artery is a superior method of measuring a person’s body temperature.
We are so used to living with mild diseases that cause fevers, that self-medication with over-the-counter (OTC) drugs, such as paracetamol or ibuprofen, is routine for us. However, fever in a hospital setting is a completely different matter, as it can indicate more serious threats to health or even life. Nosocomial or hospital acquired infections are serious, difficult to treat and difficult to overcome.
Whenever a fever is high, especially when onset is abrupt, the shivering, the prostration, and the discomfort along with simply touching the patient will lead to a clear diagnosis. If we need to detect fever early and when it is not so high, before the symptoms are obvious, we need a reliable, sensitive, accurate thermometer.
Thermometry plays an essential role in the early detection and treatment of these diseases as well as others that represent co-morbidities of conditions that require hospitalization. A thermometer has two objectives: to answer the question: fever yes or no and to quantify it to determine how severe it is
Ultimately, we need to make a clinical decision about whether to treat or not, and how to do so. A wide range of thermometry solutions exists that are valid and that, for the most part, have reached the status of standard of care (SOC). Among the non-invasive or minimally invasive procedures are axillary, oral, tympanic, and temporal arteries. The rectal, pulmonary artery, esophageal and bladder thermometry are invasive methods reserved for monitoring cases. Rectal thermometry is a less invasive method of these three methods and is the most commonly used among them. It is considered the gold standard in many thermometry studies.
Comfort and distress
Due to our long-lasting daily relationship with fever and thermometry, we have developed a sense of comfort with the diagnosis of fever, because using any of the SOC thermometers, anyone can answer the question: fever – yes, or no? At the same time it does not matter where we are: at home, in school, or in a hospital.
COVID-19 arrived during this period of comfort and disrupted many areas of civil and medical life. Thermometry was one of them. All of a sudden, thermometers were required even in the most unlikely places (restaurants, airports, shops, dental offices, etc.).
New vendors
Due to the high demand for thermometry and fever detection, new non-contact methods emerged. They promised a hygienic and fast way to screen febrile patients. Due to the apparent ease of use of IR guns, thermographic screens, and cameras used in non-contact methods, they have seen rapid adoption because they are passive and do not require medical training. These vendors, as well as the many new suppliers of SOC methods, were all granted the accuracy needed for fever detection automatically.
In the past two years, we have learned four key lessons. We have yet to learn and understand some important matters concerning fever and thermometry:
- Incorporating initial febrile screening with hygienic and social distancing measures is proving beneficial beyond the COVID19 pandemic, because hospital-based infectious diseases are on the decline (3).
- All thermometers are not created equal. Some SOC methods are more reliable than others. Unfortunately, in the rush to get supplies, many new suppliers have failed to meet the minimum accuracy requirements. There have been a number of countries that have had to review how they award quality certifications, thereby reducing the number of suppliers who qualify for certifications (Citation).
- Not every method is valid. Clinical applications of non-contact IR guns have flooded the market. An accurate screening for early stages of fever requires high sensitivity, the capacity of a diagnostic test to avoid false negatives. In one of the best and most recent studies, non-contact IR guns were reported to deliver a sensitivity of 60.5% (4). According to the FDA, these thermometers should not be used for fever screening. (Citation).
- Any suitable method can be misused. Users have some degree of control over SOC methods. Users can produce different readings of the same temperature depending on how well they use the instruments. Poor results can be caused by workflow pressure, overconfidence, or a lack of knowledge of the techniques. It is important to reduce user-dependent variability with any method, from the most challenging ones (tympanic) to the simplest (temporal artery).
It’s time to deal with some pending issues
By choosing methods with the highest accuracy and less user-dependent variability, we can improve the measurement of thermometry. Good thermometry does not come naturally. It requires rigorous attention to the details. The use of thermometers should be thoroughly and universally trained for the best diagnostic accuracy of this fundamental vital sign (4).
Better, more universally accepted guidelines and recommendations are needed for fever diagnosis and management. It is true that fever is a natural reaction to disease that will help fight the disease but it can also cause problems in itself. We need to know when to treat and how to treat it.
To establish better guidelines, we need more studies like the one on non-contact IR (4), but that also assess SOC methods. The scientific literature on clinical assessment of the different SOC thermometry options is very diverse methodologically, making it difficult to perform high-impact meta-analysis (5). Methodological issues arise from the fact that inter- and intra-observer variability is not reported and not taken into account in any of the available studies. This leads to different evaluations of the methods. In order to establish clear criteria for fever, understand their role and best indications in different clinical settings, and assess with precision the SOC options, solid studies must be conducted.
Thermometry options comparison
The following is a summary of some key features and benefits of the main clinical thermometry options. The ideal clinical thermometer should meet the following requirements:
- Safe. Among the factors involved are the risk of instrument damage and hygienic considerations.
- Easy to use. This is due to the high reproducibility and low variability of the results.
- Comfortable for the patient. Patients’ comfort is frequently disturbed by clinical maneuvers, adding to their natural discomfort. This is especially important for pediatric patients.
- Non-invasive. From the tympanic thermometer to the non-contact IR guns, many of the so-called “non-invasive” SOC methods are actually invasive to some degree. Deep thermometry methods through natural orifices (rectal, bladder, esophageal) are considered invasive.
- Fast. With the relative scarcity of nursing staff and the escalating demand for care, not to mention the pandemic crisis, nursing workflow optimization is of utmost importance.
- Precise. Decisions regarding clinical treatment must be made as soon as possible in the course of a disease and in an adequate manner. A fast and accurate diagnosis is dependent on the quality of vital signs.
- Cost-effective. The cost of use and the cost of ownership are often hidden costs. On the one hand, a very small expenditure with a high frequency will lead to a surprising annual cost (for example: disposables). The second component of ownership costs is the repair and replacement costs due to instrument fragility, fatigue, or low quality.

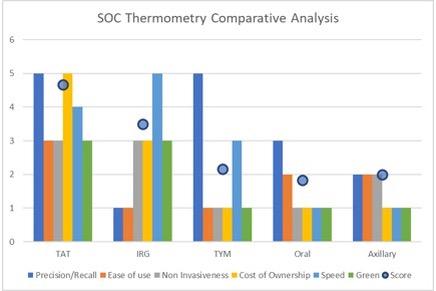
Figure 1. Comparison of the 5 main SOC non-invasive methods: TAT: Temporal Artery, IRG: Infrared guns, TYM Tympanic, Oral and Axillary. The scores are explained in the text. To help you understand the comparison we have made in figure 1, here is some context.
• The precision/recall of an instrument or method refers to its ability to correctly detect fevers with the lowest possible number of false negatives (in other words, missed fevers) and false positives (in other words, false alarms). It is an essential feature of any thermometer. In order to differentiate the methods, we have applied a multiplier to this characteristic in the scoring. A non-contact IR gun with high speed, non-invasiveness, and green values is of no use if it can’t detect a fever in 40 percent of cases.
• The first four methods (TAT, IRG, TYM, and oral) are standards of care. It means that the medical community accepts these non-invasive (minimally invasive in the case of tympanic and oral) methods as fully valid to make clinical decisions based on the results.
• All methods in figure 1 produce a different reading when compared to the gold standard central temperature (rectal, bladder, esophageal, or pulmonary artery). These differences are well documented. The difference is called ‘bias’ and it is accounted for in the hospital protocols for fever management.
• Clinically, the cutaneous temperature plays a role in specific conditions as compared with the central temperature. A very low-weight premature baby with metabolic distress is a typical example.
• Although all SOC methods are valid, they have varying degrees of variability based on the user and/or the patient. In the case of oral and axillary, this variability is related to the ease of use and the patient’s participation in the reading. By training and observing a proper technique, the variability can be minimized.
• The Temporal Artery Thermometry is the method with the highest rating. This method scores highest in all seven parameters. It is extremely easy to use it correctly, but at the same time, it is not impossible to operate it incorrectly. For any ‘easy’ vital sign collection technique, we need to follow a precise technique carefully. Patients deserve it.
References
- A. Sahib El-Radhi, Medical Journal of Islamic World Academy of Sciences 19:1, 9-14, 2011
- Green C, Krafft H, Guyatt G, Martin D (2021) Symptomatic fever management in children: A systematic review of national and international guidelines. PLoS ONE 16(6): e0245815.
- Bentivegna, E. et al. Impact of COVID-19 prevention measures on risk of health care-associated Clostridium difficile infection. Am. J. Infect. Control 49, 640–642. https:// doi. org/ 10. 1016/j. ajic. 2020. 09. 010 (2021).
- Amber S. Hussain et al. Proper use of noncontact infrared thermometry for temperature screening during COVID-19. Nature Scientific Reports | (2021) 11:11832 https://doi.org/10.1038/s41598-021-90100-1
- Geijer H, Udumyan R, Lohse G, et al. Temperature measurements with a temporal scanner: systematic review and metanalysis. BMJ Open 2016;6: e009509. doi:10.1136/ bmjopen-2015-009509
Appendix A:
Temporal Artery Thermometry
The comparison of SOC methods provided in this whitepaper suggests clear and well-defined advantages for Temporal Artery Thermometry. Exergen Corporation has developed the methodology on which Temporal Artery Thermometry is based and sell a number of Temporal Artery Thermometers based that support this SOC method.
For your reference, here is a short description of Exergen’s Temporal Artery Thermometers fir use in both large-scale hospitals, professional lite use in home care facilities, small clinics and schools, and a model for at-home use..
The Temporal Artery Thermometer is an infrared thermometer designed for accurate, completely non-invasive temperature assessment by scanning the temporal artery (TA).
Temperature is measured by gently stroking the Temporal Artery Thermometer across the forehead, and includes a momentary touch of the probe to the neck area behind the ear lobe, to account for any cooling of the forehead as a result of diaphoresis.
The patented arterial heat balance technology (AHBTM) automatically measures the temperature of the skin surface over the artery and the ambient temperature. It samples these readings some 1000 times a second, ultimately recording the highest temperature measured (peak) during the course of the measurement.
The Temporal Artery Thermometer emits nothing. It only senses the natural thermal radiation emitted from the skin.
It has been clinically proven in premier university hospitals to be more accurate than ear thermometry, and better tolerated than rectal thermometry, and is supported
by more than 100 peer-reviewed published studies covering all ages from premature infants to geriatrics in all clinical care areas. It is a superior method for patients and clinicians alike.
Three models
Exergen’s family of Temporal Artery Thermometers consists of three models:
- the TAT-5000 for use in hospitals
- the TAT-2000 for professional lite use in small clinics, schools and home-care
- the TAT-2000C for at-home use
When using a Temporal Artery Thermometer a hospital nurse, a healthcare professional or a parent measures the patient’s core body temperature by gently swiping the sensor head of the thermometer across the forehead of the patient.
Characteristics
Perfect location. The temporal artery lies just 2 millimeters under the skin on the forehead. The blood flowing through the temporal artery was just seconds before flowing through the patient’s heart, making the temporal artery a perfect spot for taking an accurate temperature measurement
Highly accurate. Both the TAT-5000 and the TAT-2000 are highly accurate thermometers. The TAT-2000 and the TAT-5000 are backed by more than 100 peer-reviewed clinical trials – the most of any professional thermometer.
Easy to use. The TAT-2000 and TAT-5000 are very easy to use. A gentle swipe of the thermometer across the forehead is all that is needed to perform a perfect measurement.
Non-invasive. By measuring the temperature of the blood in the temporal artery on the forehead, the TAT-2000 and the TAT-5000 are non-invasive. This means that patients – babies, young children, adults – will not feel intimidated. This is in contrast to rectal or ear thermometers, the use of which often causes patients discomfort.
No need to undress or move the patient. A patient’s temperature can be measured even when they are asleep. There is no need to wake them or change their position.
Very fast. It usually takes just 3-5 seconds to measure a temperature
High productivity. This combination of fast and non-invasive measurements is great for productivity. Consequently, more patients can be measured per hour and time is saved. Giving nurses and doctors more time to spend with their patients.
Very robust. Exergen’s Temporal Artery Thermometers are made of an in-house developed Superplastic.
Industrial quality. This translates into a highly attractive warranty.
Research-based. Unlike other brands, Exergen has worked with researchers and doctors around the world. Over 100 peer-reviewed clinical studies support the quality and accuracy of the Temporal Artery Thermometer.
High-quality training material. A thermometer is only as good as the person using it. Exergen has invested substantial time and money in developing high-quality training materials, both online and in print.
Recent Comments